
 简体中文
简体中文
 ENGLISH
ENGLISH


肝硬化是各种慢性肝病进展至以肝脏弥漫性纤维化、假小叶形成、肝内血管增殖为特征的病理阶段,其病因包括病毒性肝炎、酒精性肝病、脂肪性肝病、自身免疫性肝病等等,疾病进展至失代偿期,将发生肝性脑病、食管胃底静脉曲张破裂出血、肝肾综合征等严重并发症,并可能发展为肝癌,危害人体健康并给社会带来沉重的卫生经济负担。了解肝硬化的流行病学特征对于疾病防控至关重要。而肝硬化流行病学特征因地区、病因和时间不断地发生着变化。
近日,在“中华医学会肝病学分会第十四次肝纤维化、肝硬化及门脉高压学术会议”上,北京大学医学部庄辉院士分享了《我国肝硬化流行病学》精彩报告。肝胆相照平台特将主要内容整理成文,以飨读者。
一、 肝硬化流行率
一项纳入全球44项研究的Meta分析显示,一般人群肝硬化流行率为1.3%(1.12亿例),其中非洲2.8%,北美洲1.6%,拉丁美洲1.5%,亚洲1.1%,欧洲1.0%。中国的4项研究中,共计586.2354万一般人群肝硬化流行率为1.2%[1],约1000万例。
我国东北地区肝硬化流行率最高,达1.78%(图1);在575.7335万体检人群中,男性肝硬化流行率显著高于女性(1.06% vs 0.67%,P<0.001),此外,研究发现,肝硬化流行率随年龄而升高[2]。
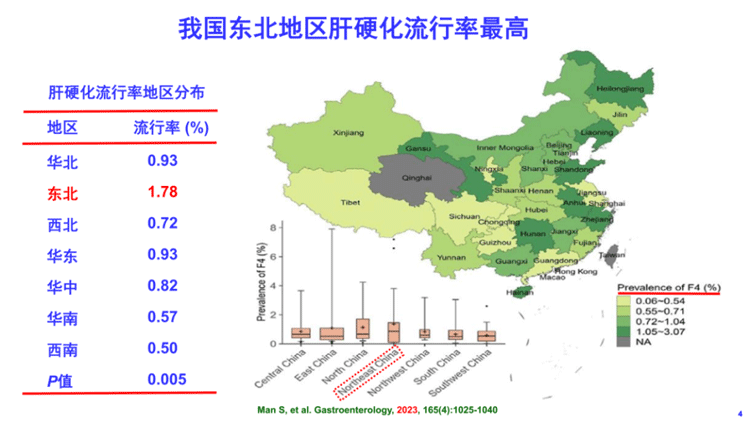
图1 我国肝硬化流行率地区分布
二、 肝硬化发病率、死亡率和伤残调整寿命年(DALYs)
1990年全球肝硬化年龄标化发病率(ASR)为25.7/10万(70万例),2019年为25.3/10万(200万例),下降了0.05%;中国1990年肝硬化ASR为27.0/10万(31万例),2019年为22.5/10万(41万例),下降了0.62%(图2)[3]。
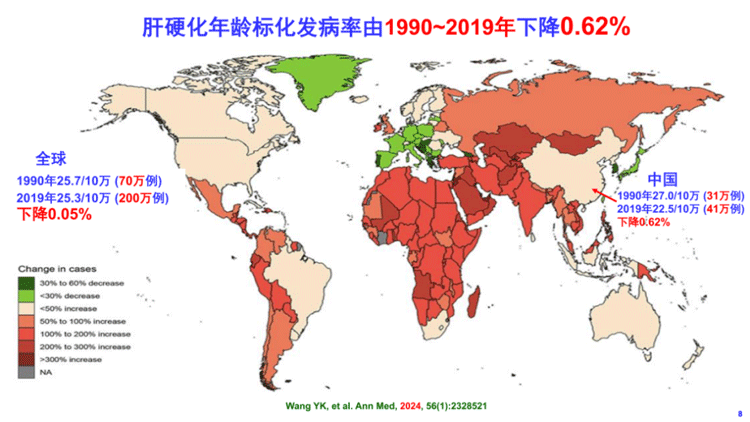
图2 肝硬化年龄标化发病率
2019年全球肝硬化年龄标化死亡率(ASDR)为18.00/10万(147.2万例);中国2019年肝硬化ASDR为7.8/10万(16万例)[3]。1990年全球肝硬化死亡顺序为第10位,2019年和2021年分别降至第11位和第12位(图3)[4]。
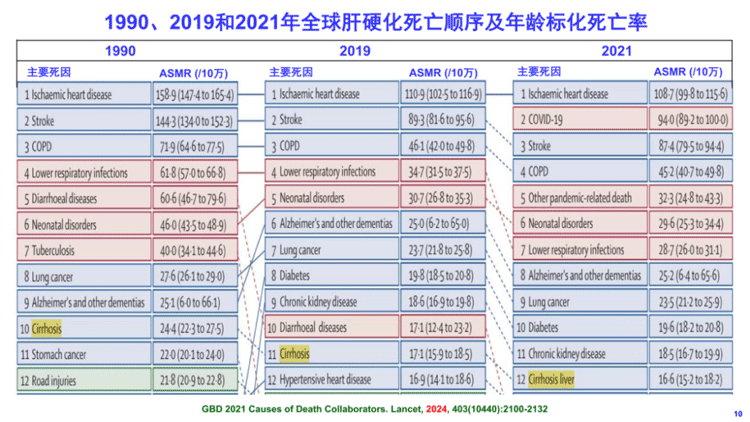
图3 全球肝硬化死亡顺序及年龄标化死亡率
1990年全球肝硬化ASDR为24.4/10万(101.3万例),2019年为18.0/10万(147.2万例),下降了42.1%;中国1990年肝硬化ASDR为8.6/10万(15万例),2019年为7.8/10万(16万例),下降了9.2%[3]。1990~2015年全球男女年龄标化死亡率均呈下降趋势(图4)[5]。
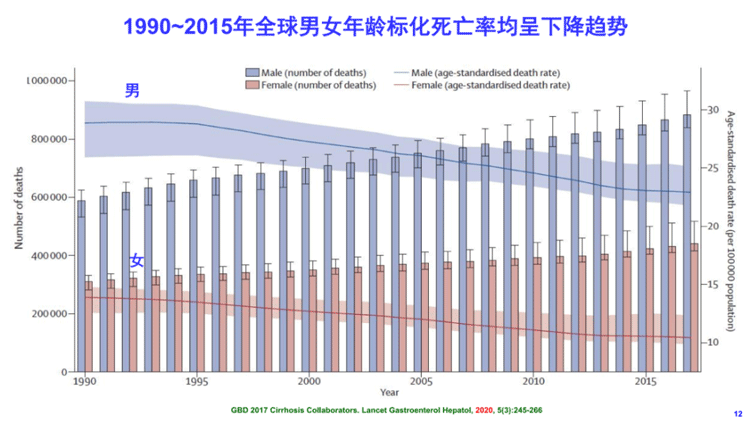
图4 1990~2015年全球男女年龄标化死亡率
2019年我国肝硬化死亡主要为45~75岁人群,25岁以下人群肝硬化死亡少见。我国男性肝硬化年龄标化死亡率(11.8/10万)较女性(4.2/10万)高1.8倍[6]。
全球肝硬化和其他慢性肝病DALYs年龄标化率为724.31/10万;中国2021年为400-799DALYs/10万[7]。
三、 肝硬化主要病因
各国肝硬化主要病因不同,北美洲以HCV感染为主,拉丁美洲、欧洲以酒精性肝病(ALD)为主,非洲不详,中国以HBV感染为主(图5)[8]。
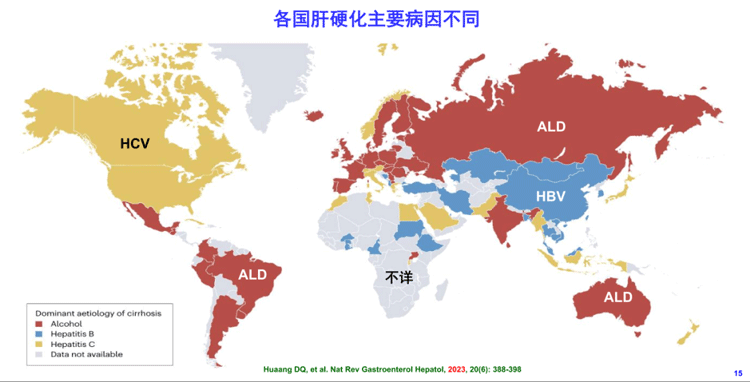
图5 各国肝硬化主要病因
1990~2019年全球和我国肝硬化病因构成发生变迁:HBV感染比例减少,NAFLD和ALD比例增加(图6)[6]。
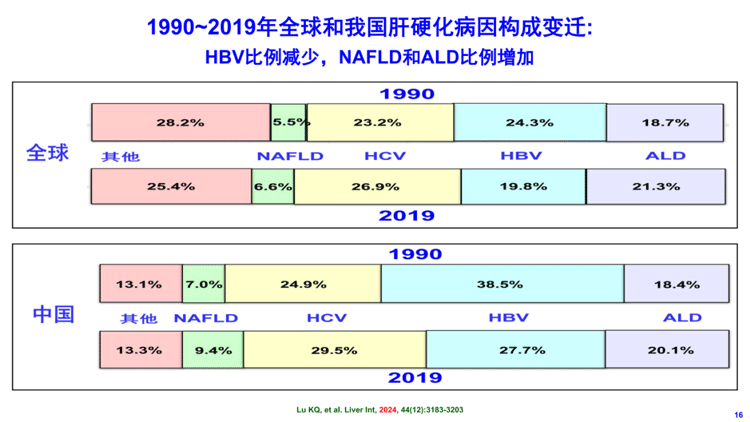
图6 肝硬化病因构成的变迁
四、 肝硬化疾病进展
代偿期肝硬化(1.12亿例)患者死亡较一般人群高5倍,每年4%~12%进展至失代偿期肝硬化(1100万例),死亡较一般人群高10倍。失代偿期肝硬化可发生腹水、肝性脑病、肝硬化心肌病、食道静脉出血、门脉高压、自发性细菌性腹膜炎、肝肺综合征、肝肾综合征、腹壁侧枝血管扩张、血小板减少症、缺铁性贫血等,并可能发展为肝细胞癌(图7)[9-16]。
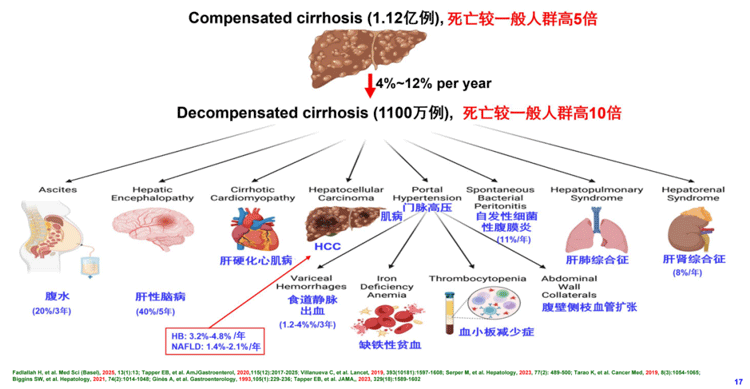
图7 肝硬化疾病进展
肝硬化进展与病因有关,HBV感染者在所有死因中15年存活率最高,达65.57%,肝病相关死亡中15年存活率达79.83%;而非肝病相关死亡中ALD患者15年存活率最高,达56.63%(表1)[17]。
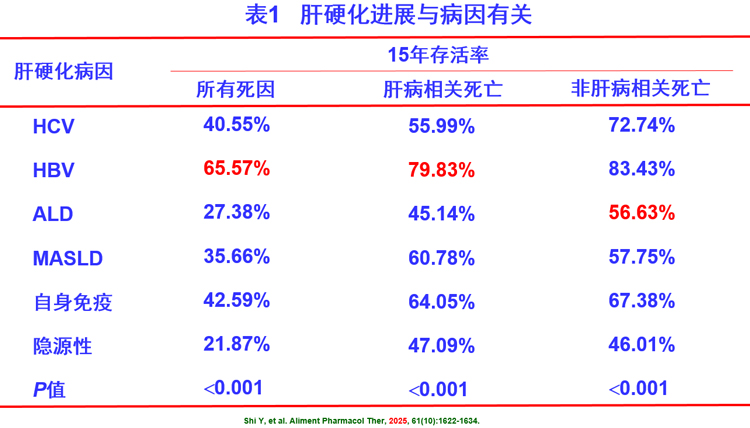
(注:HCV为HCV感染肝硬化; HBV为HBV感染肝硬化;隐源性为肝硬化)
五、小结
1. 我国肝硬化负担重:一般人群流行率为1.2%,约1000万例肝硬化;年龄标化发病率为22.5/10万,每年新发约41万例;年龄标化死亡率为7.8/10万,每年死亡约16万例;年龄标化DALYs为400~700/10万,损失伤残调整寿命年高达400~700/10万。
2. 我国肝硬化病因构成变迁:HBV感染比例减少,MAFLD和ALD比例增加。
3. 代偿性肝硬化每年4%~12%进展为失代偿期肝硬化。代偿性肝硬化死亡较一般人群高5倍,5年存活率为67%;失代偿期肝硬化死亡较一般人群高10倍,5年存活率仅45%。
【参考文献】 [1] Zamani M, Alizadeh-Tabari S, Ajmera V, et al, Loomba R. Global prevalence of advanced liver fibrosis and cirrhosis in the general population: A systematic review and meta-analysis. Clin Gastroenterol Hepatol, 2025, 23(7):1123-1134. [2] Man S, Deng Y, Ma Y, et al. Prevalence of liver steatosis and fibrosis in the general population and various high-risk populations: A nationwide study with 5.7 million adults in China. Gastroenterology, 2023, 165(4):1025-1040. [3] Wang Y, Wang M, Liu C, et al. Global burden of liver cirrhosis 1990-2019 and 20 years forecast: results from the global burden of disease study 2019. Ann Med,2024, 56(1):2328521. [4] GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet, 2024, 403(10440):2100-2132. [5] GBD 2017 Cirrhosis Collaborators. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol, 2020, 5(3):245-266. [6] Lu K, Sui J, Yu W, et al. An analysis of the burden of liver cirrhosis: Differences between the global, China, the United States and India. Liver Int, 2024, 44(12):3183-3203. [7] Tham EKJ, Tan DJH, Danpanichkul P, et al. The global burden of cirrhosis and other chronic liver diseases in 2021. Liver Int, 2025, 45(3):e70001. [8] Huang DQ, Terrault NA, Tacke F, et al. Global epidemiology of cirrhosis - aetiology, trends and predictions. Nat Rev Gastroenterol Hepatol,2023, 20(6):388-398. [9] Fadlallah H, El Masri D, Bahmad HF, et al. Update on the complications and management of liver cirrhosis. Med Sci (Basel), 2025, 13(1):13. [10] Tapper EB, Zhao L, Nikirk S, et al. Incidence and Bedside predictors of the first episode of overt hepatic encephalopathy in patients with cirrhosis. Am J Gastroenterol, 2020, 115(12):2017-2025. [11] Villanueva C, Albillos A, Genescà J, et al. β blockers to prevent decompensation of cirrhosis in patients with clinically significant portal hypertension (PREDESCI): a randomised, double-blind, placebo-controlled, multicentre trial. Lancet, 2019, 393(10181):1597-1608. [12] Serper M, Kaplan DE, Taddei TH, Tapper EB, Cohen JB, Mahmud N. Nonselective beta blockers, hepatic decompensation, and mortality in cirrhosis: A national cohort study. Hepatology, 2023, 77(2):489-500. [13] Tarao K, Nozaki A, Ikeda T, et al. Real impact of liver cirrhosis on the development of hepatocellular carcinoma in various liver diseases-meta-analytic assessment. Cancer Med, 2019, 8(3):1054-1065. [14] Biggins SW, Angeli P, Garcia-Tsao G, et al. Diagnosis, evaluation, and management of ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: 2021 practice guidance by the American Association for the Study of Liver Diseases. Hepatology, 2021,74(2):1014-1048. [15] Ginès A, Escorsell A, Ginès P, et al. Incidence, predictive factors, and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology, 1993,105(1):229-236. [16] Tapper EB, Parikh ND. Diagnosis and Management of Cirrhosis and Its Complications: A Review. JAMA, 2023, 329(18):1589-1602. [17] Shi Y, Chien N, Fong A, et al. Differential characteristics and survival outcomes of patients with cirrhosis according to underlying liver aetiology. Aliment Pharmacol Ther, 2025, 61(10):1622-1634.
整理 | 肝胆相照平台
审校 | 庄辉院士